Date: Tuesday, 26 May 2020
KEY POINTS
· East and Southern Africa is the region most affected by HIV in the world and is home to the largest number of people living with HIV.
· The HIV epidemic in this region is generalized but young women, men who have sex with men, transgender people, sex workers, prisoners and people who inject drugs are at an increased vulnerability to infection.
· Improved availability of HIV testing services now means less than two out of every ten people living with HIV are unaware of their status.
· The number of people living with HIV in East and Southern Africa continues to increase, but access to antiretroviral treatment is increasing as well.
· Although laws and cultural traditions vary between East and Southern Africa n countries, there are a number of ingrained cultural, structural and legal barriers to HIV prevention.
Explore this page to find out more about populations most affected by HIV, testing and counselling programs, prevention programs, antiretroviral treatment, civil society’s role, HIV and TB, barriers to HIV prevention, funding, and the future of HIV and AIDS in East and Southern Africa.
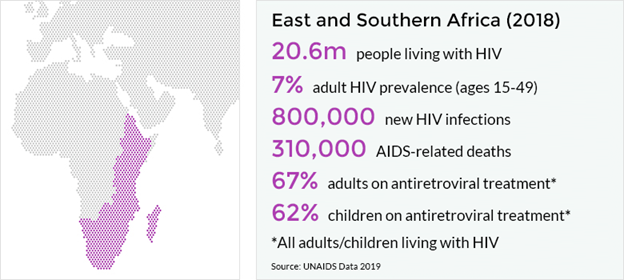
East and Southern Africa is the region hardest hit by HIV. It is home to around 6.2% of the world’s population but over half (54%) of the total number of people living with HIV in the world (20.6 million people). In 2018, there were 800,000 new HIV infections, just under half of the global total. 1
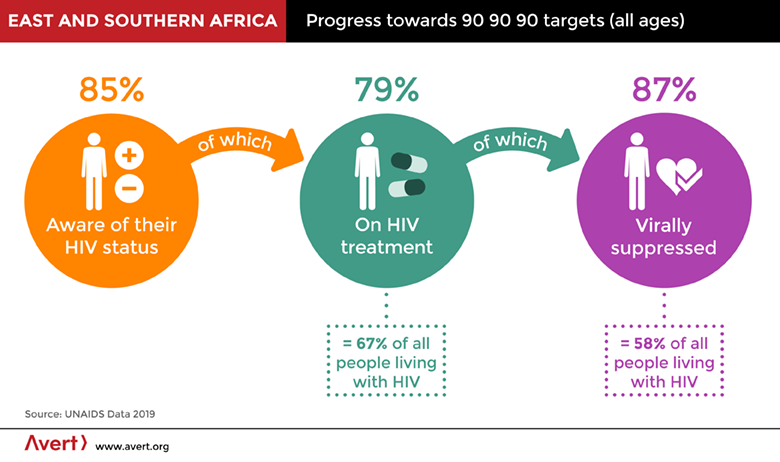
South Africa accounted for more than a quarter (240,000) of the region’s new infections in 2018. Seven other countries accounted for more than 50% of new infections: Mozambique (150,000), Tanzania (72,000), Uganda (53,000), Zambia (48,000), Kenya (46,000), Malawi (38,000), and Zimbabwe (38,000).2 Overall, new infections in the region have declined by 28% since 2010.3Around 310,000 people died of AIDS-related illnesses in the region in 2018, although the number of deaths has fallen by 44% since 2010.4Despite the continuing severity of the epidemic, huge strides have been made towards meeting the UNAIDS 90-90-90 targets. In 2018, 85% of people living with HIV were aware of their status, 79% of them were on treatment (equivalent to 67% of all people living with HIV in the region), and 87% of those on treatment had achieved viral suppression (equivalent to 58% of all people living with HIV in the region).5
Three countries (Botswana, Eswatini and Namibia) have now reached coverage of 90% or above for the three key focus areas in the HIV care cascade, and Rwanda is close. But progress is poor in other countries. For example, in Madagascar, Mauritius and South Sudan, fewer than 25% of people living with HIV are aware of their status, and eight countries in the region are still not reporting data on viral suppression.6
|
Between 2010 and 2018, new HIV infections declined among children (0-14 years) from 1.1 million to 84,000. New infections among adults declined from 930,000 to 710,000 over the same period, although there is significant variation between countries. Strong declines were seen in Comoros, Rwanda, South Africa and Uganda. But in Angola, Madagascar and South Sudan the annual number of new infections increased.7 8
Of the 19.6 million adults living with HIV in the region in 2018, 12 million are women and 7.6 million are men.9Young women (aged 15–24 years) accounted for 26% of new HIV infections in 2018, despite making up around10% of the population.10
Although East and Southern Africa’s HIV epidemic is driven by sexual transmission and is generalized, meaning it affects the population as a whole, certain groups such as sex workers and men who have sex with men have significantly higher HIV prevalence rates. For example, in 2018 Lesotho reported HIV prevalence among the general population at 23.6%, one of the highest in the world. The last recorded survey in 2014 shows prevalence is even higher among sex workers at 72% and men who have sex with men at 33%.11In 2018, 25% of new HIV infections in East and Southern Africa were among key affected populations and their sexual partners, despite these groups making up a fraction of the total population. Yet programming for key populations remains insufficient and many people from these groups face stigma, discrimination and legal barriers that prevent them from accessing HIV services.12
Groups most affected by HIV in East and Southern Africa
Young women
In 2018, HIV prevalence among young women (15-24 years) in the region was more than double that of young men (1.6 million young women living with HIV, compared to 660,000 young men), and in some countries the disparity between genders is even greater.13
The reasons behind this are numerous and complex. For example, the existence of high levels of transactional sex and age-disparate sexual relationships in many countries increase young women’s HIV vulnerability.14 Studies from Zimbabwe and Uganda, which have marriage patterns comparable with many other parts of the region, found young married women with partners who were 16 or more years older than them were at three times greater risk of HIV infection than those with partners less than15 years older than themselves.15
A 2014 UNAIDS assessment of demographic and health surveys carried out in the region suggests young women face higher levels of spousal physical or sexual violence than women from other age groups.16. Again, this heightens HIV risk – for example, a South African study found young women who experienced intimate partner violence were 50% more likely to have HIV than young women who had not experienced violence.17
Although knowledge among young people is improving it remains low in a number of countries, with young women less aware than young men. For example, in Kenya where knowledge of HIV prevention among young people is relatively high, 64% of young men have adequate knowledge, compared to 57% of young women. In Mauritius, HIV prevention knowledge is low with only a third (32%) of young people aware of how to prevent HIV. When broken down by gender, this equates to just 4% of young women, compared to 30% of young men.18
Data reported to UNAIDS suggests 80% of sexually active adolescent boys and young men (and 30% of their female counterparts) had sex with a non-married, non-cohabiting partner in the last year. In most countries, too few young people reported using condoms during these sexual encounters, with young women less likely than young men to report using condoms.19Such low levels of condom use may be partly reflective of the fact that around half of the region’s countries impose age-restrictions on buying condoms.20
Children
In 2018, 1.1 million children (0-14 years) were living with HIV in East and Southern Africa.21 The main route for HIV transmission among children is through birth (see later section on preventing mother-to-child transmission). However, the region also has high levels of underage, child and forced marriage.
In 2017, 9% of women aged 20-24 years had been married or in union by the time they were 15, while 35% of women in this age bracket had been married or in union by the age of 18.22 This equates to around 7 million child brides.23 As ever, there are regional differences. For example, in Ethiopia, 14% of women are married before they are 15 and 40% are married before they are 18. Whereas in Eswatini, 1% are married before they are 15 and 5% before they are 18.24
Girls who marry as children are more likely to be beaten or threatened by their husbands than girls who marry later. They are also more likely to describe their first sexual experience as forced. As minors, child brides are rarely able to assert their wishes, such as whether to practice safer sex.25 These factors all increase HIV risk.
Political will to curb child marriage is growing in the region. In 2015, Malawi increased the legal marriage age to 18 and in 2016 Zimbabwe outlawed child marriages.26. In 2015, Ethiopia developed a national strategy to address child marriage and female genital mutilation and has seen the prevalence of early marriage fall by a third in the past decade.27 28
Sex workers
More than half (55%) of all sex workers in the region are estimated to be living with HIV.29 Although sex workers are disproportionately affected by HIV in every country in East and Southern Africa, HIV prevalence among this population varies greatly between countries, ranging from 5.5% in Madagascar to more than 70% in Lesotho and Uganda. In Botswana, Malawi, Rwanda and Zimbabwe more than 40% of female sex workers are living with HIV.30
Although the number of new HIV infections among sex workers in 2018 was lower than among men who have sex with men in the region, the substantial (but undocumented) number of clients of sex workers who are exposed to HIV means HIV among this key population group has the greatest impact on the region’s epidemic overall.31
It is estimated that at least 90% of sex workers in the region are female, although selling sex is also common among men who have sex with men and transgender people.32 The majority of the region’s countries identify sex workers in their national HIV strategies.33 Despite this, how many sex workers are being reached with prevention and treatment is difficult to determine due to a lack of reported data.34
Condom usage by sex workers and their clients varies greatly. In some cases, sex workers have no access to condoms, have trouble negotiating their use with clients or are unaware of their importance. In other cases, police actively confiscate or destroy sex workers’ condoms. A 2012 study in Kenya, South Africa and Zimbabwe found evidence of physical and sexual abuse and harassment of sex workers who carry condoms. Police were also using the threat of arrest on the grounds of condom possession to extort and exploit sex workers.35
Modelling estimates in Kenya show that a reduction of approximately 25% of HIV infections among sex workers may be achieved when physical or sexual violence is reduced.36
Men who have sex with men (MSM)
While data on men who have sex with men (sometimes referred to as MSM) in East and Southern Africa is limited, where reported HIV prevalence ranges from 2% in Angola to 31% in Zimbabwe.37Overall, around one in five (20%) of men who have sex with men in the region are estimated to be living with HIV.38
HIV transmission between men who have sex with men accounted for 4% of new infections in the region in 2018.39 However, evidence suggests the majority of the region’s men who have sex with men also engage in heterosexual sex, often with wives or other long-term female partners.40 The HIV epidemic among men who have sex with men is therefore interlaced with the epidemic in the wider population.41
Although limited, data reported suggests condom use by men who have sex with men exceeded 70% in South Africa, Kenya and Rwanda, and was above 50% in Angola, Comoros, Eswatini, Madagascar and Mauritius. Lesotho, Malawi and Tanzania reported levels below 50% at 46%, 44% and 14% respectively.42With the exception of Botswana, Comoros and Ethiopia, all national AIDS plans or strategies in the region identify men who have sex with men as a key population. However, specific programs for this group are extremely limited and constrained by widespread homophobia and, in some countries, the criminalization of same-sex practices.43
People who inject drugs (PWID)
Kenya, Madagascar, Mauritius, Mozambique, South Africa, Tanzania and Uganda are all home to significant populations of people who inject drugs (sometimes referred to as PWID). Although regional data is limited, country surveys among people who inject drugs suggest high HIV prevalence.44 Overall, just under a third (30%) of people who inject drugs in the region are estimated to be living with HIV.45 It is estimated that this population group accounted for 8% of new HIV infections in the region in 2018.46
In Kenya, HIV prevalence among people who inject drugs was 18% in 2011, compared to 5.6% among the general population.47 In Tanzania it is estimated that 15.5% of people who inject drugs are living with HIV48, with HIV prevalence among women who inject drugs thought to be higher than among their male counterparts.49
In 2018, an estimated 21.8% of people who inject drugs in South Africa were living with HIV.50 A 2015 study in five South African cities found 32% of men and 26% of women who inject drugs regularly shared syringes and other injecting equipment and nearly half reused needles.51
Evidence from Kenya, Mauritius, Seychelles and Tanzania suggests many people who inject drugs acquire HIV before the age of 25.52
Prisoners and HIV in East and Southern Africa
Although data is limited, East and Southern Africa is thought to have one of the highest rates of HIV prevalence among prisoners in the world at just under 30%.53 This is reflective of high HIV prevalence in the general population and the continued criminalization of key population groups. It is also due to the fact that prisons are high risk environments for HIV transmission, fueled by over-crowding, limited access to health care, drug use, unsafe injecting practices, sexual violence, unprotected sex and tattooing.54
Transgender people
The only country in the region to report national data on transgender people is Mauritius where 28.4% of this population group were estimated to be living with HIV.55 Elsewhere, HIV prevalence among transgender people is thought to be extremely high.56 Improving data – and disaggregating data on transgender people from data relating to men who have sex with men – is critical to improve health outcomes for this group.
HIV testing and counselling (HTC) in East and Southern Africa
In recent years, a number of countries in the region such as Botswana, Kenya, Uganda, Malawi and Rwanda have implemented national campaigns to encourage uptake of HIV testing and counselling (HTC). In 2018, 85% of people living with HIV had knowledge about their status – a significant improvement from 77% in 2015 and higher than the global percentage in 2018 (79%).57 58
Access to HTC has been a major barrier to testing up-take and a number of strategies have been used to address this. Provider-initiated testing remains the region’s main approach, but community-based testing is growing as it has been shown to be effective in reaching large numbers of first-time testers, diagnosing people living with HIV at earlier stages of infection, and linking those who test positive to care. Workplace and door-to-door testing, using rapid diagnostic tests, is also increasing.59
Increasing HIV self-testing in East and Southern Africa
HIV-related stigma remains a huge barrier to testing, something that self-testing kits may help to side step. In 2015, Kenya announced plans to introduce self-test kits.60In the same year, self-testing began in Malawi, Zambia and Zimbabwe through the four-year Unit aid STAR (Self-Testing Africa Research) Initiative; the largest ever evaluation of self-testing.
STAR’s second phase expanded self-testing access to Eswatini, Lesotho and South Africa. By November 2018 the Initiative had distributed 2.3 million HIV self-test kits in these countries. It significantly increased HIV testing coverage, particularly among men, young people and first-time testers.61 STAR has also been shown to improve the proportion of key populations testing positive who then access treatment.62
I decided to get tested so that I could be aware of my HIV status. I have big dreams that I would like to achieve in life like everybody else and I want to stay healthy and prevent myself from HIV infection. I also encourage my friends and fellow young people to go for HIV testing regularly and take control of their lives.
- Keisha Eldred Mushi, HTC participant, Dar es Salaam, Tanzania63
HIV prevention programs in East and Southern Africa
In 2018, around 800,000 people in East and Southern Africa were newly infected with HIV.64A number of countries in the region have conducted large-scale prevention programs in an effort to contain and reduce their HIV epidemics. In 2015, Ethiopia, Malawi, Eswatini and Zimbabwe began to revitalize their national prevention programs. In the same year, Kenya, Zimbabwe and South Africa began developing a regional roadmap to accelerate scale-up of combination HIV prevention services at local levels and increase investments for combination HIV prevention.65. This has now been translated into a number of national roadmaps.
Often new infections and HIV prevalence are located among particular locations and populations. As a result, a number of countries in the region are developing sub-national HIV estimates to apply a location and population approach to HIV prevention. For example, in Kenya 65% of new HIV infections are in just 9 out of 47 counties. The country’s new HIV Prevention Roadmap reflects this by targeting interventions to specific geographical areas and, to some extent, populations.66
Despite this helpful development, and the fact that all national strategic plans in the region mention key populations67, insufficient attention is still being given to people most affected by HIV. For example, nearly 1 million sex workers across the region are thought to be in need of HIV prevention services. Programmed coverage ranges from 38% in South Sudan to 74% in Kenya.68
Programmed for young women
In 2013 ministers of health and education from countries across the region committed to bringing in a raft of programs to address the barriers that prevent girls and young women from accessing services. Focuses include keeping girls in school, comprehensive sexuality education, girl-friendly sexual and reproductive health (SRH) services, eliminating gender-based violence and female genital mutilation, and economic and political empowerment.69
DREAMS
DREAMS aimed to reduce HIV infections among adolescent girls and young women by 40% in Kenya, Lesotho, Malawi, Mozambique, South Africa, Eswatini, Tanzania, Uganda, Zambia, and Zimbabwe between 2015-2017/18. The programmed focused on social isolation, economic disadvantage, discriminatory cultural norms, orphan hood, gender-based violence and education.70
In 2016, the South African government created She Conquers, a national campaign to implement the DREAMS programmed beyond the districts already being supported. Also in 2016, Eswatini partnered with the Global Fund and the National Emergency Response Council on HIV/AIDS, resulting in close to national coverage on HIV prevention for adolescent girls and young women.71
Data on DREAM’s impact from one the programmer’s main donors, the U.S. President’s Emergency Plan for AIDS Relief (PEPFAR), suggests that communities or districts involved in DREAMS which had the highest HIV burdens when the programmed began had seen new HIV diagnoses among young women decline by between 25% to 40% as of 2017.72 Additional evaluation of DREAM’s immediate and longer-term impact continues.73
Preventing HIV among adolescents in East and Southern Africa
UNAIDS and UNICEF’s All in to End Adolescent AIDS (All In) also works to reduce new HIV infections among young women. All In aims to motivate governments and partners to collaborate across sectors in order to accelerate the HIV response for adolescents (10-19 years). It also prioritizes the meaningful involvement of adolescents in the HIV response, enabling adolescents and young people to lead, design and evaluate programs.
All In began in 2015 in 25 priority countries, 14 of which are in the region. By 2018 it had resulted in more targeted prevention programming for adolescents, better data, more funding, and seen adolescents play key roles in the HIV response at sub-national level.74
It has been an eye opener. We need to look at adolescents separately and target our programs accordingly.
- Ketlaantshang Monyadiwa, District AIDS Coordinator, Botswana.75
Condom availability and use
Condom availability varies widely by country, with only five countries meeting the United Nations Population Fund (UNFPA) regional benchmark of 30 male condoms distributed per man per year between 2011 and 2014.76 Overall in 2015 in sub-Saharan Africa (regional-specific data unavailable), the estimated condom need was six billion male condoms, but only about 2.7 billion condoms were distributed.77
Condom use at last sex among adults with more than one sexual partner in the past 12 months is low, estimated at 23% among men and 33% among women in 2015. 78 However, condom use varies substantially among countries. In 2018, it ranged from 13% among men in Madagascar to 85% among men in Zimbabwe. Among women, it ranged from 5% in Madagascar to 76% in Lesotho.79 Condom use among men who pay for sex is generally higher, at about 60%.80
HIV education and approach to sex education
In 2013, 20 countries in the region committed to improving sexual and reproductive education for young people. In 2016 governments reaffirmed this commitment and agreed on a roadmap that would enable 95% of adolescents and young people (10-24 years) to have comprehensive HIV prevention knowledge by 2020.81
As of July 2019, 14 countries had achieved one of the key indicators – providing comprehensive sexuality education (CSE) and life skills in at least 40% of primary and secondary schools. All were implementing CSE training programs for teachers.82However, there are questions surrounding the quality of information, teaching and training in some contexts.83
A number of HIV prevention awareness campaigns targeting adults have also proven successful including the multi-country One Love campaign and South Africa’s Love-Life.84
Prevention of mother-to-child transmission (PMTCT)
Significant progress has been made in the prevention of mother-to-child transmission (PMTCT) of HIV in East and Southern Africa.
Between 2010 and 2018, new HIV infections among children (0-14 years) fell from 170,000 to 84,000.85
The general decline in infections is due to the rapid increase in PMTCT services. In 2018, 92% of HIV positive pregnant women received ART to protect their health and prevent HIV transmission to their infant. In 2010, just half (49%) of pregnant women in the region received PMTCT services.86
As ever there is country variation. In 2018, Botswana, Malawi, Mauritius, Mozambique, Namibia, Rwanda and Zambia were enabling more than 95% of pregnant women living with HIV to access effective ART. Close to this target, with coverage above 90%, were Ethiopia, Kenya, Uganda, Tanzania and Zimbabwe. At the other end of the scale, in Madagascar 25% of pregnant women were accessing ART, and in Angola 38% were.87
Progress on PMTCT could be further improved by improving access to point-of-care HIV testing for infants (‘early infant diagnosis’), which reached 68% of at-risk infants in 2018.88
Voluntary medical male circumcision (VMMC)
In 2007, the World Health Organization (WHO) and UNAIDS recommended voluntary medical male circumcision (VMMC) as a key component of HIV prevention in countries with a generalized epidemic, following the discovery that male circumcision could reduce the risk of sexual transmission of HIV from females to males by 60%.
In response, VMMC accelerated rapidly in the region between 2008 and 2014, reaching 3.2 million circumcisions per year. In 2015 and 2016 this fell to around 2.6 million circumcisions then rose again in 2018 to 4.1 million. Trends vary between provinces and countries. For instance, more than 70% of adult men are circumcised in Tanzania, the Gambela region of Ethiopia, Lesotho and the Nyanza province of Kenya. In Zimbabwe, fewer than one in four adult men are circumcised.89
Harm reduction
Harm reduction interventions that help prevent HIV transmission, such as needle and syringe programs (NSPs), education on safe injecting practices and opioid substitution therapy (OST), exist on a relatively small scale in the region but they are growing. Although limited, Kenya, Mauritius, South Africa and Tanzania all offer NSP and OST services. Uganda and Mozambique are piloting NSPs and the Seychelles has one OST site.90
Kenya and South Africa are leading the way on scaling up harm reduction programmes.91] For example, Kenya introduced NSPs and OST in 2012. As of 2017, there were 19 NSP sites operating in the country. Although these services fail to reach everyone who needs them, there are approximately 135 needles distributed per person who injects drugs per year, a substantial increase on 2015 levels.92
Pre-exposure prophylaxis (PrEP)
In 2015, South Africa became the first country in the region to fully approve pre-exposure prophylaxis (PrEP), the use of antiretroviral drugs to protect HIV-negative people from HIV before potential exposure to the virus. A month later, Kenya followed suit, specifically with young women and girls in high-incidence areas. 93 Since then, Zimbabwe, Zambia, Uganda, Namibia, Mozambique, Mauritius, Lesotho and Botswana have all begun introducing PrEP, mainly through trials or demonstration projects.94
It is estimated that around 84,000 people in the region took PrEP at least once in 2018.95 PrEP use is highest in Kenya, at more than 31,000 people, followed by South Africa (around 8,000), Uganda and Lesotho (around 7,000 each).96
As evidence grows showing the effectiveness and acceptability of PrEP, particularly for key populations and those unable to negotiate condom use, rollout is accelerating.
HELP US HELP OTHERS
Avert.org is helping to prevent the spread of HIV and improve sexual health by giving people trusted, up-to date information.
We provide all this for FREE, but it takes time and money to keep Avert.org going.
Can you support us and protect our future?
Every contribution helps, no matter how small.
Antiretroviral treatment (ART) in East and Southern Africa
Antiretroviral treatment (ART) programs have been scaled-up dramatically in East and Southern Africa over the past decade.
In 2018, there were an estimated 13.8 million people on ART in region. This is more than a three-fold increase from 2010 numbers and represents 67% of all people living with HIV in East and Southern Africa.97 98
More women than men are on treatment as men are less likely to test for HIV and are more likely to interrupt or drop out of treatment. In 2018, 72% of all adult women living with HIV were on treatment, compared to 59% of HIV positive men.99 Consequently, men in the region are more likely than women to die of AIDS-related causes despite being less likely than women to acquire HIV.100
This disparity is partly due to harmful gender norms that prevent men from seeking help, accepting care or admitting to having a highly-stigmatized condition such as HIV.101
In 2018, the proportion of children living with HIV on treatment increased to 62% from 22% in 2010. In the same year, 60% or more of children living with HIV were on ART in Eswatini, Kenya, Lesotho, Malawi, Mozambique, Namibia, Rwanda, South Africa, Uganda, Tanzania, Zimbabwe and Zambia. At the other end of the scale, only 5% of HIV positive children in Madagascar, 9% in South Sudan and 13% in Angola were on treatment.102
All countries in the region are at least implementing 2013 WHO treatment guidelines, which expanded eligibility for ART for people with a CD4 count of 500 or less. Kenya, Malawi, Namibia, Uganda, Lesotho, Botswana, South Africa, Zambia, South Sudan, Eswatini and Ethiopia have adopted the 2015 WHO guidelines to immediately offer treatment to people diagnosed with HIV, known as ‘test and treat’ or ‘treat all’.103
A study assessing the change in the proportion of people staring treatment within 30 days of enrolment in HIV care after six countries adopted test and treat policies found the rate of ART initiation had sharply accelerated in Malawi, Uganda, and Zambia, slowed in Kenya and had not changed in Rwanda and Burundi.104
Although South Africa has the largest number of people (4.8 million) with HIV on ART, its reaches just 62% of those who need treatment, coverage that falls below the regional average.105 In 2018, treatment coverage was highest in Botswana (83%), Eswatini (86%), Namibia (92%), Rwanda (87%) and Zimbabwe (88%).106
Weak health and community systems continue to undermine the effective scale-up of test and treat approaches. Further gaps in the provision of treatment are caused by humanitarian emergencies and food insecurity in some places. As a result, 58% of all people living with HIV in East and Southern Africa in 2018 had achieved the viral suppression necessary to prevent onward HIV transmission.107However, Botswana, Eswatini, Rwanda and Namibia have achieved the 2020 target of 73% viral suppression (set by UNAIDS)..108Data reported to UNAIDS from 12 countries in the region showed that about 44% of people accessing ART in East and Southern Africa accessed routine viral load testing in 2016 – key to monitoring ART effectiveness.109
In the first ever qualitative study on viral load monitoring and suppression in a rural African setting, a study from Mozambique found viral load monitoring to be highly valued by people living with HIV and their healthcare workers. However, it found evidence of misinformation and communication challenges around what the results mean for people’s health. It also found that limited health system resources resulted in delays to people receiving test results, which made viral failure difficult to manage clinically, while disempowering and frustrating both patients and health workers.110
Civil society’s role in East and Southern Africa
Many civil society organizations (CSOs) were set up in response to the HIV epidemic and continue to play a critical role in the region’s response today.
A significant proportion of CSOs are led by the communities they serve and as a result are better able to reach people living with HIV and key populations. Many are engaged in SRH service delivery and advocacy.111
Funding for civil society, particularly community-led groups, has tended to come from international donors, and has been dwindling since the 2008 global economic recession.112 The United States of America’s reintroduction in 2017 of the Mexico City policy, also known as the ‘global gag rule’, which blocks US funds to any overseas organization involved in abortion advice and care, has also resulted in further funding cuts for many CSOs working on HIV and sexual and reproductive health in the region.113 Repressive laws against drug use, sex work and same sex relations also constrain the actions of many CSOs concerned with the rights and health of key populations.
Encouragingly, national and regional support for civil society has been growing in recent years, with UNAIDS reporting increasing interest from several governments in understanding the unique contributions community groups have in addressing HIV.114 115
HIV and tuberculosis (TB) in East and Southern Africa
In 2016, ten countries in the region (Angola, Ethiopia, Kenya, Lesotho, Mozambique, Namibia, South Africa, Tanzania, Zambia and Zimbabwe) were classified by WHO as being among the 30 countries with the highest tuberculosis (TB) burden.116
TB is a leading cause of death for people living with HIV. Overall, 180,000 people with HIV died of TB-related deaths in 2018. Although this number is steadily falling, the region accounts for more than half the total number of TB-related deaths among people living with HIV in the world (300,000).117
The main reason the number of HIV/TB-related deaths in East and Southern Africa is decreasing is due to the expansion of ART and the integration of HIV/TB services. Overall, 85% of people known to have TB/HIV co-infection were on ART in Eswatini, Kenya, Malawi, Mozambique, Namibia, Uganda and Tanzania as of 2017. In contrast, in Angola and Botswana the proportion is less than half.118
South Africa has made gains in providing people living with HIV with isoniazid preventative therapy (IPT), which stops people from developing active TB. More than more than half (53%) of diagnosed HIV positive people in South Africa now have access to this. Ethiopia and Eritrea are also providing increased IPT coverage, at 46% and 38% respectively but IPT is not sufficiently accessible in the rest of the region.119
Barriers to the HIV response in East and Southern Africa
Stigma and discrimination
HIV-related stigma and discrimination remains a major barrier to tackling HIV in East and Southern Africa. Cultural beliefs about HIV and AIDS around contamination, sexuality and religion have played a crucial role in the development of HIV-related discrimination.120 For example, in Ethiopia more than half of people surveyed said they would avoid buying vegetables from someone living with HIV and 42% said children living with HIV should not be allowed to go to school with other children. In other countries, stigmatizing attitudes expressed by survey participants ranges from 6% to 31%121
Moreover, studies have shown that HIV-related stigma remains pervasive within healthcare, with health workers’ negative and discriminatory views towards HIV-positive people influenced by, and often similar to, those in the general population.122 In Mauritius, one in three people living with HIV have been denied health services due to being HIV positive. In Uganda, a survey among people who inject drugs found almost two thirds (64%) avoided healthcare services for fear of discrimination or of being reported to law enforcement authorities.123
The region remains a largely hostile environment for men who have sex with men, sex workers, transgender people, and people who use drugs. People from key affected populations often experience heightened levels of stigma and discrimination as a result. This often prevents people from accessing HIV services.124 For example, many sex workers do not wish to disclose their occupation to healthcare providers and consider stigma and discrimination a major barrier to HIV testing.125
The status of women
Women and girls in the region often face discrimination in terms of access to education, employment and healthcare. Men often dominate heterosexual relationships, and gender-based violence levels are high, especially for young women.126 Around 30% of women in South Africa, Uganda and Tanzania; 25% in Angola, Kenya and Zambia and 20% in Ethiopia, Malawi, Namibia, Rwanda and Zimbabwe are estimated to have experienced physical and/or sexual violence by an intimate partner in the past 12 months.127
Legal barriers
Overly broad criminalization of HIV exposure, non-disclosure and transmission in the region continues to stigmatize people living with HIV, which undermines public health initiatives, and is ultimately damaging to HIV prevention.128The criminalization of sex work, drug use, and same sex practices, as well as the lack of legal recognition of gender identity, compounds key affected populations’ inability to access HIV services.129 Among countries in the region, 13 criminalize some aspect of sex work, 12 criminalize same-sex relationships, 15 criminalize HIV exposure, non-disclosure and transmission, and 3 specifically criminalize transgender people.130
However, some progress has been made with both the Seychelles and Mozambique repealing provisions that criminalize sex between men in 2016.131 In 2019, Botswana also decriminalized same-sex relations. However, in Kenya in the same year, a long legal battle to recognize the laws used to criminalize LGBT people as unconstitutional was rejected.132Human Rights Watch (24 May 2019) ‘Kenya: Court Upholds Archaic Anti-Homosexuality Laws’ (accessed July 2019)
Structural and resource barriers
A number of areas with high HIV prevalence, particularly rural areas, have a lack of healthcare workers. This is due to a lack of funding for healthcare, coupled with a continual ‘brain drain’ of healthcare staff from the region to high-income countries, and an internal ‘brain drain’ from rural to urban areas, and from the public to private sector. To overcome the lack of qualified workforce, many countries have implemented task-shifting programs and given community health care workers increasing responsibilities.133 134
Data issues
Despite key populations being disproportionately affected by HIV in the region, data on these groups remains lacking. This makes targeting interventions that address key population needs, or charting the success of such programs, extremely difficult.
Data collection and monitoring of people living with HIV is important for improving the consistency of care people receive, which ultimately helps people adhere to treatment. However, many countries in the region do not have such systems in place due to a lack of technical capacity, human resource availability and coordination. For example, eight do not report data on viral suppression.135This lack of comprehensive data makes it hard to track people across prevention and treatment services and can leads to inaccuracies in reported data.136
However, a number of countries are starting to address this including Botswana, Eswatini, Tanzania and Namibia.137
In addition, an analysis of available data between 2000 and 2017 revealed widespread differences in the prevalence of HIV across and within countries. The study found substantial differences in both the direction and rate of change in HIV prevalence, highlighting the degree to which important local differences are masked when examining trends at the country level.138
Funding for HIV in East and Southern Africa
Between 2010 and 2018, domestic and international resources for HIV responses in the region grew by 34% and 31%, respectively. However, between 2017 and 2018, the total amount of available resources fell by 7% (after adjusting for inflation). This is the result of domestic funds decreasing by 9%, US bilateral funding decreasing by 2%, Global Fund money decreasing by 29%, and funding from all other international channels decreasing by 10%.
South Africa now funds the majority of its HIV response domestically, covering 78% of all costs. Zambia, Zimbabwe, Kenya and Malawi are also significantly increasing their domestic investments. However, when South Africa is excluded, only 20% of the HIV response in the region is funded domestically. Countries will need to mobilize almost US$ 800 million in additional resources by 2020 to fully fund an effective HIV response.139
The future of HIV and AIDS in East and Southern Africa
Tackling the HIV epidemic in East and Southern Africa is a long-term task that requires sustained effort and planning from both domestic governments and the international community.
In order to meet UNAIDS’ 2020 targets, between 2019 and 2020 the region must diagnose 1.1 million people living with HIV who did not previously know their HIV status, start an additional 3 million people on ART, and ensure an additional 3 million people living with HIV achieve viral suppression.140
Girls and young women must be placed at the center of the response if the region is to drastically reduce HIV. This means meaningfully addressing gender inequality and inequity, tackling harmful traditional practices such as child marriage, and increasing educational opportunities.141
Insufficient financial resources, combined with the lack of strategic information, has led to many high-impact HIV prevention programs not being implemented to the necessary standard or scale in the region. These systems must be strengthened to enable the region’s HIV response to be evidence-based, and ultimately more effective.
Countries in East and Southern Africa will need to assess how to allocate what are currently limited resources. For example, increased linkages between sexual and reproductive health (SRH) and HIV services have been shown to increase access and uptake for both SRH and HIV services. Using the skills of civil society organizations and the ability of communities most affected by HIV to implement services will be crucial to achieving effective results with limited resources.
Fundamental barriers to treatment, particularly HIV-related stigma and discrimination and HIV-specific criminal legislation, must also be overcome. Removing such barriers would encourage more people to get tested and seek out treatment, reducing the burden of HIV across the region. The increasing impact of migration also needs to be prioritized, as people move between and within countries, creating changing patterns of healthcare needs.142
Serious challenges remain in terms of key affected populations, including the criminalization of same-sex sexual relations, drug use and sex work, insufficient implementation of harm-reduction programs, and insufficient protection of people from discrimination, harassment, violence and abuse arising from sexual orientation or gender identity. In many countries the prioritization of key populations within national AIDS plans and strategies has not resulted in sufficient financial allocation and programmed implementation to address their needs.143However, in some countries, key affected community networks are emerging and regional networks now exist for female sex workers and men who have sex with men. These networks are essential to strengthen the response for key affected populations.144 145
|
Last updated:
31 October 2019
Last full review:
31 October 2019
Next full review:
31 October 2022